Disability Premium Triggered by Diagnostic Code Not Lost Workday Log
Since the early 2000s, disability insurance claims turned on a single document: the lost workday log. An adjuster cross-referenced dates, verified medical notes, and decided whether the policyholder truly could not work. That process is being replaced by something far simpler: a match between a diagnostic code in an electronic health record and a policy's trigger list. No log, no adjuster, no waiting. The claim pays automatically.
The Claim Check: Why Disability Insurers Are Betting on ICD-10, Not Pay Stubs
Traditional disability insurance relies on proof of lost income. The policyholder submits pay stubs, doctor's notes, and a signed attending physician statement. The carrier then adjudicates whether the condition meets the policy's definition of disability — usually an inability to perform the material duties of one's occupation. This process is slow, expensive, and prone to leakage. A 2024 study by the Society of Actuaries, titled "Administrative Leakage in Disability Claims," estimated that up to 15% of claim dollars go to administrative costs or overpayment due to subjective judgment.
New parametric disability products skip that entire chain. Instead of requiring proof of lost workdays, they pay a fixed benefit when a specific diagnostic code appears in the policyholder's electronic health record. The trigger is binary: the code is present, or it is not. No human adjudicator weighs evidence. The policy language shifts from "inability to work" to "code confirmed." This changes the underwriter's job from evaluating medical history to mapping which codes are worth covering and at what benefit level.
The shift is not hypothetical. The Hartford, Cigna, and MetLife have filed parametric disability riders with state regulators since 2023. RenaissanceRe told ReinsuranceNe.ws in early 2025 that it had seen a "material uptick" in demand for diagnostic-code-based coverage from group life and disability writers. The appeal is clear: faster claims, lower expense ratios, and reduced exposure to moral hazard. But the trade-off is basis risk — the code may not perfectly capture the severity or duration of the condition.
For the actuary, this is a new pricing frontier. Traditional disability tables group risks by occupation class and age. Parametric models require granular data on how often each ICD-10 code appears in a given population, how long it typically persists, and how frequently it leads to wage loss. The output is not a premium per thousand of covered payroll but a premium per code trigger. Reinsurers are demanding code-level experience data before they will assume the tail risk. Lockton's recent 12% revenue rise, driven partly by its reinsurance brokerage, reflects growing intermediary demand for this kind of structured data.
How a Single Alphanumeric Code Replaces the Attending Physician Statement
ICD-10-CM codes are the backbone of medical billing in the United States. Every diagnosis a physician records in an electronic health record maps to a code like M54.5 (low back pain) or I10 (essential hypertension). These codes are standardized, machine-readable, and already flowing through healthcare data pipelines. For a parametric disability product, the carrier simply specifies a list of covered codes. When the policyholder is diagnosed with a condition on that list, the electronic health record feed triggers an automatic payout.
No faxed forms, no waiting for a doctor to sign an attending physician statement. The claim is filed and paid within days, sometimes hours. For conditions like fractures, appendicitis, or myocardial infarction — where the code is unambiguous and the clinical course is well understood — this works well. The carrier knows the expected recovery window and can set the benefit duration accordingly. The loss ratio improves because leakage from overpayment or fraudulent malingering is eliminated. There is no opportunity to exaggerate symptoms or extend absence beyond medical necessity.
But the attending physician statement served a purpose beyond verification: it provided context. A code does not tell the insurer whether the patient has comorbidities, whether the condition is acute or chronic, or whether the treatment plan is aggressive or conservative. Carriers address this by limiting the benefit to a fixed amount per code, not a percentage of salary. The policyholder gets a lump sum or a fixed monthly payment for a predefined period, regardless of actual wage loss. This is indemnity turned into index.
The actuarial challenge is to price that index correctly. A carrier offering a $10,000 lump sum for diagnosis of acute myocardial infarction (I21.0) needs to know the frequency of that code in the insured population and the probability that the condition will cause a prolonged work absence. The frequency data can come from public health databases or proprietary claims experience, but the link between code and work absence is less well documented. Early parametric products have relied on conservative assumptions, pricing in a margin to account for uncertainty.
The Parametric Shift: From Indemnity to Index-Based Payouts
Parametric insurance is not new. It has been used for decades in weather and crop insurance, where a payout is triggered when a rainfall index or temperature threshold is crossed. The key feature is that the payout is based on an objective, verifiable parameter, not on actual loss. This eliminates the need for loss adjustment and speeds up claims. The same logic now applies to disability: the diagnostic code is the parameter, and the benefit is fixed.
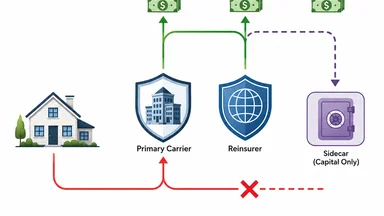
The shift from indemnity to index changes the insurer's risk profile. Under traditional disability insurance, the carrier bears the risk of both the occurrence of a condition and the duration of the resulting work absence. Under parametric disability, the carrier bears only the risk of the code's occurrence. The duration risk is transferred to the policyholder, who receives a fixed benefit regardless of how long they are actually out of work. This is a cleaner risk to model and to reinsure.
The trade-off between speed and precision is inherent. For a healthy 30-year-old who breaks a leg skiing, a parametric trigger on code S82.0 (fracture of patella) might pay $5,000 — enough to cover a few weeks of lost income. For a 55-year-old with a herniated disc that requires surgery and months of recovery, the same code trigger might be inadequate. Carriers are experimenting with code-plus-duration triggers, where the benefit escalates if the code persists beyond a certain date. That reintroduces some of the complexity parametric insurance was meant to eliminate.
Data Partnerships: The Unseen Infrastructure Behind the Trigger
For a diagnostic code trigger to work, the insurer needs real-time access to the policyholder's electronic health record. This requires data-sharing agreements with electronic health record vendors, hospital systems, and health information exchanges. The technical standard is HL7 FHIR (Fast Healthcare Interoperability Resources), which enables real-time streaming of discrete data elements like diagnosis codes. Patient consent is collected at policy issue, typically through a HIPAA-compliant authorization that allows the carrier to query the patient's record for covered codes only.
Smaller insurers often lack the infrastructure to build direct integrations with multiple EHR systems. They license code maps from third-party vendors like MRO or Health Catalyst, which maintain connections to thousands of healthcare providers. These vendors de-identify the data before passing it to the carrier, adding a layer of privacy protection. The carrier never sees the full medical record — only the code that triggered the claim. This reduces the carrier's exposure to protected health information and simplifies compliance.
The data partnership model is still maturing. Some carriers report latency of 24 to 72 hours between a diagnosis being recorded and the code appearing in the insurer's system. For acute conditions like stroke or heart attack, that delay is acceptable. For conditions diagnosed in an outpatient setting, the delay can be longer because the record may not be updated until the physician closes the encounter. Carriers are negotiating service-level agreements that guarantee code availability within a set window, and some are building direct feeds from large hospital networks to reduce latency.
Reinsurers are watching these partnerships closely. The quality of the data pipeline directly affects the accuracy of claims experience. If codes are missing or delayed, the carrier may underreport incidence and misprice the product. Lockton's reinsurance growth, reported at 12% in fiscal 2026, suggests that brokers are helping carriers structure data-sharing agreements that satisfy reinsurer due diligence. The infrastructure is becoming a competitive differentiator.
Pricing the Code: Actuarial Tables Based on Diagnostic Incidence
Traditional disability insurance pricing relies on occupation class, age, gender, and benefit period. The actuary uses a morbidity table that shows claim incidence and termination rates by these factors. Parametric disability pricing requires a different set of inputs: code frequency, code duration distributions, and the probability that a code will lead to a claim under the policy's trigger rules. The actuary builds a transition matrix that shows how often a policyholder moves from one code to another over time.
For example, a policy that covers code M54.5 (low back pain) must account for the fact that many people with low back pain also receive code M51.2 (lumbar disc displacement) within weeks. The benefit may be triggered by either code, so the actuary needs to model the correlation between them. This is more complex than traditional morbidity modeling because the code space is vast — there are over 72,000 ICD-10-CM codes — and many codes are rarely used in a working-age population. Carriers typically limit their trigger lists to a few hundred codes that account for the majority of short-term disability claims.
Reinsurers are demanding granular code-level experience data before they will assume the tail risk. A standard reinsurance treaty for traditional disability covers all claims above a certain attachment point. For parametric disability, the reinsurer wants to know the expected frequency and severity for each covered code. Some reinsurers have built their own code-level databases using public health surveys and commercial claims data. Lockton's reinsurance division has been active in helping carriers compile and present this data to reinsurers.
The pricing models are still in their early stages. Some carriers use a simple frequency-severity approach, multiplying the expected number of code occurrences by a fixed benefit amount. Others use more sophisticated stochastic models that simulate the progression of codes over time. The Society of Actuaries published a working paper in 2025 that proposed a framework for pricing parametric disability, but there is no industry standard yet. Prices vary widely across carriers, reflecting different assumptions about code frequency and basis risk.
The Blind Spots: Conditions That Don't Map Cleanly
Not all conditions map neatly to a diagnostic code trigger. Mental health disorders, for example, are coded under the F00–F99 range, but the codes are subjective. A diagnosis of major depressive disorder (F32.2) depends on the clinician's judgment, not a lab test. Two patients with identical symptoms might receive different codes from different providers. Carriers are wary of covering mental health codes because of the difficulty in verifying the diagnosis and the potential for adverse selection. Some cap mental health benefits at a lower amount or require a second code, such as a GAF score, to validate severity.
Chronic pain codes are another blind spot. Low back pain (M54.5) is one of the most common disability claims, but it is also one of the most subjective. Studies have shown that the same patient may receive different codes for back pain from different physicians, depending on whether imaging was performed. Carriers that cover M54.5 typically limit the benefit to a short duration, such as 30 days, to avoid paying for chronic conditions that are hard to diagnose objectively. Some exclude it entirely.
Cancer staging codes change during treatment. A patient diagnosed with breast cancer may start with code C50.9 (malignant neoplasm of breast, unspecified) and later receive code C79.5 (secondary malignant neoplasm of bone) if the cancer metastasizes. The parametric trigger must account for code progression. Some carriers pay a single benefit at initial diagnosis and then a second benefit if the code changes to a metastatic stage. Others pay a single benefit at any point during the treatment period, regardless of code changes. The actuarial treatment of cancer codes is still evolving.
Maternity codes have predictable but variable duration. Normal delivery (O80) typically results in a recovery period of six to eight weeks, but complications can extend that. Carriers that cover maternity codes must decide whether to pay a flat benefit regardless of delivery type or to differentiate between vaginal delivery and cesarean section (O82). The trade-off is between simplicity and fairness. Most parametric maternity products pay a flat benefit that approximates the average recovery cost, leaving the policyholder to bear the risk of a longer recovery.
What This Means for the Broker and the Buyer
For brokers, the shift to diagnostic code triggers means learning a new vocabulary. Instead of comparing policy definitions of disability, they must understand which ICD-10 codes are covered, what the benefit amount is per code, and whether there are any duration caps. A broker selling a parametric disability rider to a small business must explain that the policy pays $2,000 for a broken leg but nothing for a back strain that keeps the employee out of work for a month. The conversation is about code lists, not policy wordings.
For buyers, the appeal is speed and simplicity. A claim that used to take weeks can now be paid in days. But the coverage is narrower. A parametric policy does not cover every condition that might cause work absence. It covers only the conditions on the trigger list. Buyers must decide whether the trade-off is worth it. Some group plans are adopting parametric disability as a supplemental layer on top of traditional indemnity coverage. The parametric layer pays a quick lump sum for common conditions, while the traditional layer covers longer absences from any cause.
Embedded disability products — those sold through employer portals or as add-ons to life insurance — are natural fits for the parametric model. The buyer does not need to answer detailed health questions; the policy is issued based on age and occupation. The trigger is transparent: if you get diagnosed with one of these codes, you get paid. The Hartford, for example, has been experimenting with embedded parametric disability for its group life clients. At RISKWORLD 2026, The Hartford's Matt Scott discussed a new workplace violence product, but the company's broader digital strategy includes parametric triggers for common disability events.
Whether the diagnostic code trigger becomes a permanent fixture or a transitional experiment depends on the quality of experience data that will accumulate over the next three to five years. Early loss ratios are promising but based on thin exposure. If basis risk proves manageable and policyholder satisfaction remains high, the parametric model may expand into longer-duration coverages. If claims disputes shift from medical verification to code interpretation, the industry may need to revisit the simplicity that made parametric triggers attractive. The answer will come from the numbers, not from marketing. Reinsurers and actuaries will be watching closely.
This article is for informational purposes only and does not constitute professional actuarial, legal, or insurance advice. Readers should consult qualified professionals for advice tailored to their specific circumstances.